How Do You Treat Bursitis Of The Foot?
Overview
Achilles tendon bursitis is inflammation of the fluid-filled sac (bursa) located either between the skin of the back of the heel and the Achilles tendon (posterior Achilles tendon bursitis) or in front of the attachment of the Achilles tendon to the heel bone (anterior Achilles tendon bursitis, retrocalcaneal bursitis). Typical symptoms include swelling and warmth and a tender spot at the back of the heel. The diagnosis is based on symptoms, an examination, and sometimes x-rays. Treatment is aimed at relieving the inflammation and, depending on the location of the Achilles tendon bursitis, eliminating the pressure on the back of the heel. The Achilles tendon is the tendon that attaches the calf muscles to the heel bone. Posterior Achilles tendon bursitis is often associated with formation of a bone prominence called Haglund deformity or ?pump bump? on the heel bone. Anterior Achilles tendon bursitis is also called Albert disease or retromalleolar bursitis.
Causes
Certain medical conditions and medications suppress people's immune systems and make them more susceptible to septic bursitis. For example, people with cancer, HIV/AIDS, lupus, alcoholism, chronic obstructive pulmonary disease (COPD), and diabetes may be more likely to get septic bursitis. History of inflammation of the bursa. Patients who have had bursitis in the past have an increased chance of getting it again. There may be more than one reason why the retrocalcaneal bursa is inflamed. In these cases, treatment should address all of the causes.
Symptoms
Symptoms include pain at the back of the heel, especially when running uphill or on soft surfaces. There will be tenderness and swelling at the back of the heel which may make it difficult to wear certain shoes. When pressing in with the fingers both sides are the back of the heel a spongy resistance may be felt.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
Long Term Treatment must be directed towards eliminating the abnormal tilting of the heel, regardless of its cause. If this is delayed, the usual results are the pain and swelling becomes worse, chronic, and debilitating. Eventually, painful calcifications and bone spur formations may occur on the back of the heel, along with tears in the Achilles Tendon. These are serious problems that may require surgical intervention. In order to eliminate abnormal heel tilt, the foot must be re-balanced. Controlling and reducing the biomechanical foot defects that are causing the heel to tilt best accomplish this. The "Gold Standard" of medical care (that treatment most used by doctors and therapists) to help eliminate pain, inflammation, and swelling at the back of the heel is orthotics.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Achilles tendon bursitis is inflammation of the fluid-filled sac (bursa) located either between the skin of the back of the heel and the Achilles tendon (posterior Achilles tendon bursitis) or in front of the attachment of the Achilles tendon to the heel bone (anterior Achilles tendon bursitis, retrocalcaneal bursitis). Typical symptoms include swelling and warmth and a tender spot at the back of the heel. The diagnosis is based on symptoms, an examination, and sometimes x-rays. Treatment is aimed at relieving the inflammation and, depending on the location of the Achilles tendon bursitis, eliminating the pressure on the back of the heel. The Achilles tendon is the tendon that attaches the calf muscles to the heel bone. Posterior Achilles tendon bursitis is often associated with formation of a bone prominence called Haglund deformity or ?pump bump? on the heel bone. Anterior Achilles tendon bursitis is also called Albert disease or retromalleolar bursitis.
Causes
Certain medical conditions and medications suppress people's immune systems and make them more susceptible to septic bursitis. For example, people with cancer, HIV/AIDS, lupus, alcoholism, chronic obstructive pulmonary disease (COPD), and diabetes may be more likely to get septic bursitis. History of inflammation of the bursa. Patients who have had bursitis in the past have an increased chance of getting it again. There may be more than one reason why the retrocalcaneal bursa is inflamed. In these cases, treatment should address all of the causes.
Symptoms
Symptoms include pain at the back of the heel, especially when running uphill or on soft surfaces. There will be tenderness and swelling at the back of the heel which may make it difficult to wear certain shoes. When pressing in with the fingers both sides are the back of the heel a spongy resistance may be felt.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
Long Term Treatment must be directed towards eliminating the abnormal tilting of the heel, regardless of its cause. If this is delayed, the usual results are the pain and swelling becomes worse, chronic, and debilitating. Eventually, painful calcifications and bone spur formations may occur on the back of the heel, along with tears in the Achilles Tendon. These are serious problems that may require surgical intervention. In order to eliminate abnormal heel tilt, the foot must be re-balanced. Controlling and reducing the biomechanical foot defects that are causing the heel to tilt best accomplish this. The "Gold Standard" of medical care (that treatment most used by doctors and therapists) to help eliminate pain, inflammation, and swelling at the back of the heel is orthotics.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Treatment For Hammer Toe Pain
 Overview
Overview
A hammertoes occurs when the joint of the toes curl down. The reason they curl abnormally is due to a muscle imbalance which results in the tendons becoming unnaturally tight. They are due to Heredity, improper shoes, and Arthritis. There are two types of hammer toes, flexible or rigid. These classification are based on the mobility of the toe joints. A flexible hammer toe is one with a flexible toe joint that allows it to be straightend with your finger. In time a flexible joint may turn into a rigid hammer toe. Normally flexible hammer toes are much less painful than rigid hammer toes. A rigid hammer toe is one with a rigid toe joint, one that is not moveable with your finger. These rigid toe joints can be very painful and limit the ability to move.
Causes
While most cases of hammertoes are caused by an underying muscle imbalance, it may develop as a result of several different causes, including arthritis, a hereditary condition, an injury, or ill-fitting shoes. In some cases, patients develop hammertoes after wearing shoes or stockings that are too tight for long periods of time. These patients usually develop hammertoes in both feet.
 Symptoms
Symptoms
Common reasons patients seek treatment for toe problems are toe pain on the knuckle. Thick toe calluses. Interference with walking/activities. Difficulty fitting shoes. Worsening toe deformity. Pain at the ball of the foot. Unsightly appearance. Toe deformities (contractures) come in varying degrees of severity, from slight to severe. The can be present in conjunction with a bunion, and develop onto a severe disfiguring foot deformity. Advanced cases, the toe can dislocate on top of the foot. Depending on your overall health, symptoms and severity of the hammer toe, the condition may be treated conservatively and/or with surgery.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your hammertoe symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
Wear wide shoes with plenty of room in the toes and resilient soles. Avoid wearing shoes with pointed toes. Commercially available felt pads or cushions may ease pressure from the shoe on the toe. Toe caps (small, padded sleeves that fit around the tip of the toe) may relieve the pain of hammer toe. Do toe exercises, to help toe muscles become stronger and more flexible.
Arch supports or an orthotic shoe insert prescribed by your doctor or podiatrist may help to redistribute weight on the foot. These devices do not cure the problem but may ease the symptoms of either hammer toe or mallet toe.
Surgical Treatment
Treatment of a severe hammertoe that has become rigid includes surgery. What is done during the surgery depends on how misshapen and inflexible the toe is. The surgeon may make a cut over your toe and release the tendon by cutting the tendon away from the bone. The surgeon may remove a small piece of bone from the toe. The surgeon may realign the tendons to reposition your toe or fasten the bones with pins. Sometimes the surgeon may have to join the bones in the toe. In this case, you will no longer be able to bend the toe, but the toe will be flat.
Do Bunions Call For Surgery
Overview
 Bunions are a common problem that most people experience as a bony protuberance at the base of the big toe. A bunion, however, is more complicated than simply a bump on the foot. When a patient has a bunion, the big toe angles in toward the other toes, a condition called hallux valgus. Bunions are most common in women, and the cause is most often unsuitable footwear.
Bunions are a common problem that most people experience as a bony protuberance at the base of the big toe. A bunion, however, is more complicated than simply a bump on the foot. When a patient has a bunion, the big toe angles in toward the other toes, a condition called hallux valgus. Bunions are most common in women, and the cause is most often unsuitable footwear.
Causes
Bunions are most often caused by an inherited faulty mechanical structure of the foot. This faulty structure causes the drifting of the great toe and the bone to become prominent on the side of the foot. The skin then gets pinches by this bony prominence and the shoe. Therefore in most cases bunions are not caused by tight shoes but are made more painful by tight shoes. End stage bunions may become painful both in and out of shoes.
Symptoms
The major symptom of bunions is a hard bump on the outside edge of the foot or at the base of the big toe. Redness, pain and swelling surrounding or at the MTP joint can also occur.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
One of the best things you can do is to go for wider, deeper shoes. Trevor Prior says there should be a centimeter between the end of your longest toe and end of shoe. You should also choose shoes with an adjustable strap or lace. Podiatrists often recommend exercises to strengthen muscles and tendons around the big toe. Here?s one you can try yourself. Put your feet side by side, and try to move your big toes towards each other. Do this three or four times a day, while you?re in the bath or in bed. 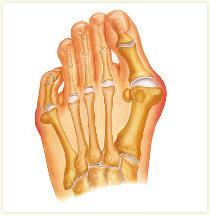
Surgical Treatment
Bunion surgery is most often performed as an out-patient, this means you go home that same day. It will likely be done at a hospital or out-patient (ambulatory) surgery center. The anesthetic choices with bunion surgery are local with sedation, spinal or general anesthesia. You wouldn?t expect that a small bunion would be treated exactly the same as a large one. Over the years, surgeons have developed dozens of methods to surgically correct bunions. But don?t worry because only a handful of methods are used today. With most bunion surgeries today, the procedure involves a combination of soft-tissue rebalancing of ligaments and tendons as well as bone work to re-align the foot structure. You may have heard people say they had their ?bunion shaved.? In most cases, the surgery often involves much more than simply shaving the bunion. The shaving part of the procedure is called an ?exostectomy? and often performed in conjunction with other methods.
Prevention
Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes.
Is Overpronation
Overview
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
During our development, the muscles, ligaments, and other soft tissue structures that hold our bones together at the joints become looser than normal. When the bones are not held tightly in place, the joints are not aligned properly, and the foot gradually turns outward at the ankle, causing the inner ankle bone to appear more prominent. The foot moves in this direction because it is the path of least resistance. It is more difficult for the foot to move in the opposite direction (this is called supination). As we develop, the muscles and ligaments accommodate to this abnormal alignment. By the time growth is complete, the pronated foot is: abnormally flexible, flat, and its outer border appears raised so that as you step down you do not come down equally across the entire foot; instead, you come down mostly on the inner border of the foot. Normal aging will produce further laxity of our muscles that causes the pronation to become gradually worse.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.
Non Surgical Treatment
Get a gait analysis of your running style, this will highlight if you overpronate, oversupinate or have a neutral gait. Most podiatrists, physio's and sports therapists will offer this service, as do some specialist sports shops. Find a clinic. If you overpronate, get orthotics with extra medial support. Many running shoes have a harder material on the inside of the midsole (the thick hard foam part of the running shoe). This means the inside of the shoe will be compressed less under load and support the inside of the foot preventing it from rolling in or flattening. For people with considerable overpronation, another option is to have an orthotic device fitted. Orthotic insoles come in many types and prices. Some are pre-molded and can be bought off the shelf. These are ok for the majority of problem feet. However some cases may require specially casted orthotics from a relevant sports injury therapist or podiatrist.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
During our development, the muscles, ligaments, and other soft tissue structures that hold our bones together at the joints become looser than normal. When the bones are not held tightly in place, the joints are not aligned properly, and the foot gradually turns outward at the ankle, causing the inner ankle bone to appear more prominent. The foot moves in this direction because it is the path of least resistance. It is more difficult for the foot to move in the opposite direction (this is called supination). As we develop, the muscles and ligaments accommodate to this abnormal alignment. By the time growth is complete, the pronated foot is: abnormally flexible, flat, and its outer border appears raised so that as you step down you do not come down equally across the entire foot; instead, you come down mostly on the inner border of the foot. Normal aging will produce further laxity of our muscles that causes the pronation to become gradually worse.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.
Non Surgical Treatment
Get a gait analysis of your running style, this will highlight if you overpronate, oversupinate or have a neutral gait. Most podiatrists, physio's and sports therapists will offer this service, as do some specialist sports shops. Find a clinic. If you overpronate, get orthotics with extra medial support. Many running shoes have a harder material on the inside of the midsole (the thick hard foam part of the running shoe). This means the inside of the shoe will be compressed less under load and support the inside of the foot preventing it from rolling in or flattening. For people with considerable overpronation, another option is to have an orthotic device fitted. Orthotic insoles come in many types and prices. Some are pre-molded and can be bought off the shelf. These are ok for the majority of problem feet. However some cases may require specially casted orthotics from a relevant sports injury therapist or podiatrist.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Should I Take Care Of Severs Disease In The Home?
Overview
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the heel bone (calcaneus) and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or minor trauma from sports participation. This condition is most common in children ages 9 to 14 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease can mimic Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone. Feet that flatten out to excess (hyperpronate) are also prone to this problem, as this can involve extra torque on the calcaneus by the Achilles tendon.
Causes
Heel pain can also be caused by a stress fracture in the heel, bursitis, tendonitis, bone cysts, and rheumatologic disorders. If the athlete is not active in impact sports or is not between age 9 and 13 years, other conditions should be considered.
Symptoms
Symptoms of calcaneal apophysitis may include Pain in the back or bottom of the heel, Limping, Walking on toes, Difficulty running, jumping, or participating in usual activities or sports, Pain when the sides of the heel are squeezed.
Diagnosis
Radiography. Most of the time radiographs are not helpful because the calcaneal apophysis is frequently fragmented and dense in normal children. But they can be used to exclude other traumas. Ultrasonography. could show the fragmentation of secondary nucleus of ossification of the calcaneus in severs?s disease. This is a safe diagnostic tool since there is no radiation. This diagnostic tool can also be used to exclude Achilles tendinitis and/or retrocalcaneal bursitis.
Non Surgical Treatment
Your child's healthcare provider will ask about your child's symptoms and examine your child's feet and heels. Any of the following may be done to treat your child's pain. NSAIDs help decrease swelling and pain or fever. This medicine is available with or without a doctor's order. NSAIDs can cause stomach bleeding or kidney problems in certain people. If your child takes blood thinner medicine, always ask if NSAIDs are safe for him. Always read the medicine label and follow directions. Do not give these medicines to children under 6 months of age without direction from your child's doctor. Acetaminophen decreases pain and fever. It is available without a doctor's order. Ask how much your child should take and how often to take it. Follow directions. Acetaminophen can cause liver damage if not taken correctly. Rest will decrease swelling, and keep the heel pain from getting worse. Your child may need to decrease his regular training or exercise. He may need to completely stop running and doing other activities that put pressure on his heel until his heel pain is gone. Ask your child's healthcare provider about activities that do not put pressure on the heel. Ice should be applied on your child's heel for 15 to 20 minutes every hour or as directed. Use an ice pack, or put crushed ice in a plastic bag. Cover it with a towel. Ice helps prevent tissue damage and decreases swelling and pain. Stretching and strengthening exercises may be recommended. A healthcare provider may teach your child exercises to stretch the hamstring and calf muscles and the tendons on the back of the leg. Other exercises will help strengthen the muscles on the front of the lower leg. Your child may be told to stop exercising if he feels any pain. Shoe inserts may be needed. Your child's healthcare provider may give you heel pads or cups for your child's shoes to decrease pressure on the heel bone. You may also be given shoe inserts with firm arch support and a heel lift. Make sure your child wears good quality shoes with padded soles. Your child should not walk barefoot. An elastic wrap or compression stocking may be needed. Your child's healthcare provider may want your child to use a wrap or stocking to help decrease swelling and pain. Ask how to apply the wrap or stocking.
Prevention
Can Calcaneal Apophysitis Be Prevented? The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Sever's Disease, also known as calcaneal apophysitis, is a disease of the growth plate of the heel bone (calcaneus) and is characterized by pain in the heel of a child's foot, typically brought on by some form of injury or minor trauma from sports participation. This condition is most common in children ages 9 to 14 and is frequently seen in active soccer, football, or baseball players. Sport shoes with cleats are also known to aggravate the condition. The disease can mimic Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon contributes to Sever's Disease by pulling excessively on the growth plate of the heel bone. Feet that flatten out to excess (hyperpronate) are also prone to this problem, as this can involve extra torque on the calcaneus by the Achilles tendon.
Causes
Heel pain can also be caused by a stress fracture in the heel, bursitis, tendonitis, bone cysts, and rheumatologic disorders. If the athlete is not active in impact sports or is not between age 9 and 13 years, other conditions should be considered.
Symptoms
Symptoms of calcaneal apophysitis may include Pain in the back or bottom of the heel, Limping, Walking on toes, Difficulty running, jumping, or participating in usual activities or sports, Pain when the sides of the heel are squeezed.
Diagnosis
Radiography. Most of the time radiographs are not helpful because the calcaneal apophysis is frequently fragmented and dense in normal children. But they can be used to exclude other traumas. Ultrasonography. could show the fragmentation of secondary nucleus of ossification of the calcaneus in severs?s disease. This is a safe diagnostic tool since there is no radiation. This diagnostic tool can also be used to exclude Achilles tendinitis and/or retrocalcaneal bursitis.
Non Surgical Treatment
Your child's healthcare provider will ask about your child's symptoms and examine your child's feet and heels. Any of the following may be done to treat your child's pain. NSAIDs help decrease swelling and pain or fever. This medicine is available with or without a doctor's order. NSAIDs can cause stomach bleeding or kidney problems in certain people. If your child takes blood thinner medicine, always ask if NSAIDs are safe for him. Always read the medicine label and follow directions. Do not give these medicines to children under 6 months of age without direction from your child's doctor. Acetaminophen decreases pain and fever. It is available without a doctor's order. Ask how much your child should take and how often to take it. Follow directions. Acetaminophen can cause liver damage if not taken correctly. Rest will decrease swelling, and keep the heel pain from getting worse. Your child may need to decrease his regular training or exercise. He may need to completely stop running and doing other activities that put pressure on his heel until his heel pain is gone. Ask your child's healthcare provider about activities that do not put pressure on the heel. Ice should be applied on your child's heel for 15 to 20 minutes every hour or as directed. Use an ice pack, or put crushed ice in a plastic bag. Cover it with a towel. Ice helps prevent tissue damage and decreases swelling and pain. Stretching and strengthening exercises may be recommended. A healthcare provider may teach your child exercises to stretch the hamstring and calf muscles and the tendons on the back of the leg. Other exercises will help strengthen the muscles on the front of the lower leg. Your child may be told to stop exercising if he feels any pain. Shoe inserts may be needed. Your child's healthcare provider may give you heel pads or cups for your child's shoes to decrease pressure on the heel bone. You may also be given shoe inserts with firm arch support and a heel lift. Make sure your child wears good quality shoes with padded soles. Your child should not walk barefoot. An elastic wrap or compression stocking may be needed. Your child's healthcare provider may want your child to use a wrap or stocking to help decrease swelling and pain. Ask how to apply the wrap or stocking.
Prevention
Can Calcaneal Apophysitis Be Prevented? The chances of a child developing heel pain can be reduced by avoiding obesity. Choosing well-constructed, supportive shoes that are appropriate for the child?s activity. Avoiding or limiting wearing of cleated athletic shoes. Avoiding activity beyond a child?s ability.
Symptoms Of Flat Feet In Adults
Overview
Adult Acquired Flatfoot occurs when the arch of your foot collapses after your skeleton has stopped growing, usually resulting in the foot ?falling? inward with the toes pointing out. This allows your entire sole to touch the ground when you stand, instead of just the outside area. Arches fall for many reasons, including arthritis, injury to the supporting tendons or bones, nerve problems, diabetic collapse, pregnancy, aging, and obesity. A fallen arch doesn?t have to be painful-though as it develops and worsens, it can lead to strain and weakness in the feet that could allow for more uncomfortable foot problems later. Diabetics can develop serious complications from their fallen arches, and need to have their condition evaluated and treated. 
Causes
Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
The adult acquired flatfoot is best treated early. Accurate assessment by your doctor will determine which treatment is suitable for you. Reduce your level of activity and follow the RICE regime. R - rest as often as you are able. Refrain from activity that will worsen your condition, such as sports and walking. I - ice, apply to the affected area, ensure you protect the area from frostbite by applying a towel over the foot before using the ice pack. C - compression, a Tubigrip or elasticated support bandage may be applied to relieve symptoms and ease pain and discomfort. E - elevate the affected foot to reduce painful swelling. You will be prescribed pain relief in the form of non-steroidal antiinflammatory medications (if you do not suffer with allergies or are asthmatic). Immobilisation of your affected foot - this will involve you having a below the knee cast for four to eight weeks. In certain circumstances it is possible for you to have a removable boot instead of a cast. A member of the foot and ankle team will advise as to whether this option is suitable for you. Footwear is important - it is advisable to wear flat sturdy lace-up shoes, for example, trainers or boots. This will not only support your foot, but will also accommodate orthoses (shoe inserts). 
Surgical Treatment
If conservative treatment fails to provide relief of pain and disability then surgery is considered. Numerous factors determine whether a patient is a surgical candidate. They include age, obesity, diabetes, vascular status, and the ability to be compliant with post-operative care. Surgery usually requires a prolonged period of nonweightbearing immobilization. Total recovery ranges from 3 months to one year. Clinical, x-ray, and MRI examination are all used to select the appropriate surgical procedure.
Post Achilles Tendon Rupture Exercises
Overview  Achilles tendon ruptures commonly occur in athletic individuals in their 30s and 40s while performing activities that require sudden acceleration or changes in direction (ex. basketball, tennis, etc.). Patients usually describe a sharp pain in their heel region almost as if they were ?struck in the back of the leg?. The diagnosis of an acute Achilles tendon rupture is made on clinical examination as x-rays will reveal the ankle bones to be normal. The Achilles is the largest and strongest tendon in the body. It is subject to 2-3 times body weight during normal walking so regaining normal Achilles tendon function is critical. Achilles tendon ruptures can be successfully treated non-operatively, or operatively, but they must be treated. Surgical treatment leads to a faster recovery and a lower rate of re-rupture. However, surgery can be associated with very serious complications such as an infection or wound healing problems. For this reason non-operative treatment may be preferable in many individuals, especially those patients with diabetes, vascular disease, and those who are long-term smokers. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms A classic sign of an Achilles tendon rupture is the feeling of being hit in the Achilles are. There is often a "pop" sound. There may be little pain, but the person can not lift up onto his toes while weight bearing. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment A physical therapist teaches you exercises to help improve movement and strength, and to decrease pain. Use support devices as directed. You may need crutches or a cane for support when you walk. These devices help decrease stress and pressure on your tendon. Your caregiver will tell you how much weight you can put on your leg. Ask for more information about how to use crutches or a cane correctly. Start activity as directed. Your caregiver will tell you when it is okay to walk and play sports. You may not be able to play sports for 6 months or longer. Ask when you can go back to work or school. Do not drive until your caregiver says it is okay.
Achilles tendon ruptures commonly occur in athletic individuals in their 30s and 40s while performing activities that require sudden acceleration or changes in direction (ex. basketball, tennis, etc.). Patients usually describe a sharp pain in their heel region almost as if they were ?struck in the back of the leg?. The diagnosis of an acute Achilles tendon rupture is made on clinical examination as x-rays will reveal the ankle bones to be normal. The Achilles is the largest and strongest tendon in the body. It is subject to 2-3 times body weight during normal walking so regaining normal Achilles tendon function is critical. Achilles tendon ruptures can be successfully treated non-operatively, or operatively, but they must be treated. Surgical treatment leads to a faster recovery and a lower rate of re-rupture. However, surgery can be associated with very serious complications such as an infection or wound healing problems. For this reason non-operative treatment may be preferable in many individuals, especially those patients with diabetes, vascular disease, and those who are long-term smokers. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms A classic sign of an Achilles tendon rupture is the feeling of being hit in the Achilles are. There is often a "pop" sound. There may be little pain, but the person can not lift up onto his toes while weight bearing. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment A physical therapist teaches you exercises to help improve movement and strength, and to decrease pain. Use support devices as directed. You may need crutches or a cane for support when you walk. These devices help decrease stress and pressure on your tendon. Your caregiver will tell you how much weight you can put on your leg. Ask for more information about how to use crutches or a cane correctly. Start activity as directed. Your caregiver will tell you when it is okay to walk and play sports. You may not be able to play sports for 6 months or longer. Ask when you can go back to work or school. Do not drive until your caregiver says it is okay.  Surgical Treatment In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission. Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy.
Surgical Treatment In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission. Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy.