Do I Have Pes Planus??
Overview

Babies are often born with flat feet, which may persist well into their childhood. This occurs because children?s bones and joints are flexible, causing their feet to flatten when they stand. Young babies also have a fat pad on the inner border of their feet that hides the arch. You still can see the arch if you lift your baby up on the tips of the toes, but it disappears when he?s standing normally. The foot may also turn out, increasing the weight on the inner side and making it appear even more flat.
Causes
Turning 40 doesn?t necessarily have anything to do with it, but over time you?ve likely engaged in certain activities or developed some unhealthy habits that led to this condition. If you are overweight, you are placing excess burdens on your feet, causing the tendons to strain. Some women experience fallen arches because of weight gain during pregnancy. You also may have damaged these tendons while exercising. If you suffered a serious injury to the foot, you may have weakened the tendons, which can also lead to this development.
Symptoms
Fallen arches symptoms may include the following. Being unable to slip fingers underneath arches. Inwards rolling of foot and ankle when running. Knee problems due to lack of support from feet.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
Can you fix a fallen arch?
Non Surgical Treatment
Treatment often consists of giving the affected foot support from underneath so that the strain is taken off it (by the use of insoles or support pads) and so symptoms are relieved. A specialist in this problem is known as a podiatrist and these do work in the NHS - ask you father's doctor whether his condition is bad enough to warrant a referral to such a specialist.
Surgical Treatment

In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Babies are often born with flat feet, which may persist well into their childhood. This occurs because children?s bones and joints are flexible, causing their feet to flatten when they stand. Young babies also have a fat pad on the inner border of their feet that hides the arch. You still can see the arch if you lift your baby up on the tips of the toes, but it disappears when he?s standing normally. The foot may also turn out, increasing the weight on the inner side and making it appear even more flat.
Causes
Turning 40 doesn?t necessarily have anything to do with it, but over time you?ve likely engaged in certain activities or developed some unhealthy habits that led to this condition. If you are overweight, you are placing excess burdens on your feet, causing the tendons to strain. Some women experience fallen arches because of weight gain during pregnancy. You also may have damaged these tendons while exercising. If you suffered a serious injury to the foot, you may have weakened the tendons, which can also lead to this development.
Symptoms
Fallen arches symptoms may include the following. Being unable to slip fingers underneath arches. Inwards rolling of foot and ankle when running. Knee problems due to lack of support from feet.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
Can you fix a fallen arch?
Non Surgical Treatment
Treatment often consists of giving the affected foot support from underneath so that the strain is taken off it (by the use of insoles or support pads) and so symptoms are relieved. A specialist in this problem is known as a podiatrist and these do work in the NHS - ask you father's doctor whether his condition is bad enough to warrant a referral to such a specialist.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
True Leg Length Discrepancy Measurement
Overview
Many children have one leg that is marginally longer than the other. In most cases, the difference is present at birth but may be too slight to be detected. More significant leg length differences (more than 2 cm) often become obvious as your child grows and begins to crawl and walk. We don?t always know what causes these discrepancies. A significant discrepancy can lead to more serious problems including arthritis and difficulty walking. However, with appropriate treatment, most children with this condition can participate in regular activities. Treatment options include heel lifts and, in more severe cases, surgery to either lengthen or shorten a leg.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.

leg length discrepancy hip pain
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Many children have one leg that is marginally longer than the other. In most cases, the difference is present at birth but may be too slight to be detected. More significant leg length differences (more than 2 cm) often become obvious as your child grows and begins to crawl and walk. We don?t always know what causes these discrepancies. A significant discrepancy can lead to more serious problems including arthritis and difficulty walking. However, with appropriate treatment, most children with this condition can participate in regular activities. Treatment options include heel lifts and, in more severe cases, surgery to either lengthen or shorten a leg.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.
leg length discrepancy hip pain
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
What Are The Major Causes Of Heel Soreness
Overview

Does your heel feel painful when you get up from bed every morning, or when you get up after sitting down for a long period of time? If you often experience this sort of pain, known as ?first step pain?, you could be suffering from plantar fasciitis (pronounced fash-ee-eye-tus), an inflammation of the plantar fascia, or the band of muscle under the foot. Plantar fasciitis is the most common cause of heel pain.
Causes
If you have pain behind your heel, you may have inflamed the area where the Achilles tendon inserts into the heel bone (retrocalcaneal bursitis). People often get this by running too much or wearing shoes that rub or cut into the back of the heel. Pain behind the heel may build slowly over time, causing the skin to thicken, become red and swell. You might develop a bump on the back of your heel that feels tender and warm to the touch. The pain might flare up when you first start an activity after resting. It often hurts too much to wear normal shoes. You may need an X-ray to see if you also have a bone spur.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Treatment includes resting from the activities that caused the problem, doing certain stretching exercises, using pain medication and wearing open-back shoes. Your doctor may want you to use a 3/8" or 1/2" heel insert. Stretch your Achilles tendon by leaning forward against a wall with your foot flat on the floor and heel elevated with the insert. Use nonsteroidal anti-inflammatory medications for pain and swelling. Consider placing ice on the back of the heel to reduce inflammation.
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel spur surgery
Prevention

Make sure you wear appropriate supportive shoes. Don't over-train in sports. Make sure you warm up, cool down and undertake an exercise regime that helps maintain flexibility. Manage your weight, obesity is a factor in causing plantar fasciitis. Avoid walking and running on hard surfaces if you are prone to pain. You should follow the recognized management protocol "RICED" rest, ice, compression, elevation and diagnosis. Rest, keep off the injured ankle as much as possible. Ice, applied for 20 minutes at a time every hour as long as swelling persists. Compression, support the ankle and foot with a firmly (not tightly) wrapped elastic bandage. Elevation, keep foot above heart level to minimize bruising and swelling. Diagnosis. Consult a medical professional (such as a Podiatrist or doctor) especially if you are worried about the injury, or if the pain or swelling gets worse. If the pain or swelling has not gone down significantly within 48 hours, also seek treatment. An accurate diagnosis is essential for proper rehabilitation of moderate to severe injuries.
Does your heel feel painful when you get up from bed every morning, or when you get up after sitting down for a long period of time? If you often experience this sort of pain, known as ?first step pain?, you could be suffering from plantar fasciitis (pronounced fash-ee-eye-tus), an inflammation of the plantar fascia, or the band of muscle under the foot. Plantar fasciitis is the most common cause of heel pain.
Causes
If you have pain behind your heel, you may have inflamed the area where the Achilles tendon inserts into the heel bone (retrocalcaneal bursitis). People often get this by running too much or wearing shoes that rub or cut into the back of the heel. Pain behind the heel may build slowly over time, causing the skin to thicken, become red and swell. You might develop a bump on the back of your heel that feels tender and warm to the touch. The pain might flare up when you first start an activity after resting. It often hurts too much to wear normal shoes. You may need an X-ray to see if you also have a bone spur.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Treatment includes resting from the activities that caused the problem, doing certain stretching exercises, using pain medication and wearing open-back shoes. Your doctor may want you to use a 3/8" or 1/2" heel insert. Stretch your Achilles tendon by leaning forward against a wall with your foot flat on the floor and heel elevated with the insert. Use nonsteroidal anti-inflammatory medications for pain and swelling. Consider placing ice on the back of the heel to reduce inflammation.
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
heel spur surgery
Prevention
Make sure you wear appropriate supportive shoes. Don't over-train in sports. Make sure you warm up, cool down and undertake an exercise regime that helps maintain flexibility. Manage your weight, obesity is a factor in causing plantar fasciitis. Avoid walking and running on hard surfaces if you are prone to pain. You should follow the recognized management protocol "RICED" rest, ice, compression, elevation and diagnosis. Rest, keep off the injured ankle as much as possible. Ice, applied for 20 minutes at a time every hour as long as swelling persists. Compression, support the ankle and foot with a firmly (not tightly) wrapped elastic bandage. Elevation, keep foot above heart level to minimize bruising and swelling. Diagnosis. Consult a medical professional (such as a Podiatrist or doctor) especially if you are worried about the injury, or if the pain or swelling gets worse. If the pain or swelling has not gone down significantly within 48 hours, also seek treatment. An accurate diagnosis is essential for proper rehabilitation of moderate to severe injuries.
Limb Length Discrepancy Running
Overview
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Causes
There are many causes of leg length discrepancy. Some include, A broken leg bone may lead to a leg length discrepancy if it heals in a shortened position. This is more likely if the bone was broken in many pieces. It also is more likely if skin and muscle tissue around the bone were severely injured and exposed, as in an open fracture. Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. A break in a child's bone through the growth center near the end of the bone may cause slower growth, resulting in a shorter leg. Bone infections that occur in children while they are growing may cause a significant leg length discrepancy. This is especially true if the infection happens in infancy. Inflammation of joints during growth may cause unequal leg length. One example is juvenile arthritis. Bone diseases may cause leg length discrepancy, as well. Examples are, Neurofibromatosis, Multiple hereditary exostoses, Ollier disease. Other causes include inflammation (arthritis) and neurologic conditions. Sometimes the cause of leg length discrepancy is unknown, particularly in cases involving underdevelopment of the inner or outer side of the leg, or partial overgrowth of one side of the body. These conditions are usually present at birth, but the leg length difference may be too small to be detected. As the child grows, the leg length discrepancy increases and becomes more noticeable. In underdevelopment, one of the two bones between the knee and the ankle is abnormally short. There also may be related foot or knee problems. Hemihypertrophy (one side too big) or hemiatrophy (one side too small) are rare leg length discrepancy conditions. In these conditions, the arm and leg on one side of the body are either longer or shorter than the arm and leg on the other side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This is known as an "idiopathic" difference.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
A personalized approach to leg length discrepancy treatment works best for each patient. Your child's doctor will consider many factors when deciding on a course of treatment for this condition. Such factors can include your child's age, extent of the leg length discrepancy, medical history, how your child tolerates certain treatments and procedures, your child's health and prognosis, growth rate, and parental preferences. There is no cookie cutter treatment for each child, or even each centimeter of leg difference. Once all of these factors have been carefully considered, your child's physician will come up with an appropriate course of care. In situations of a very small leg length discrepancy, no treatment, only periodic medical evaluation, may be necessary.

how to grow taller at 17
Surgical Treatment
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Causes
There are many causes of leg length discrepancy. Some include, A broken leg bone may lead to a leg length discrepancy if it heals in a shortened position. This is more likely if the bone was broken in many pieces. It also is more likely if skin and muscle tissue around the bone were severely injured and exposed, as in an open fracture. Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. A break in a child's bone through the growth center near the end of the bone may cause slower growth, resulting in a shorter leg. Bone infections that occur in children while they are growing may cause a significant leg length discrepancy. This is especially true if the infection happens in infancy. Inflammation of joints during growth may cause unequal leg length. One example is juvenile arthritis. Bone diseases may cause leg length discrepancy, as well. Examples are, Neurofibromatosis, Multiple hereditary exostoses, Ollier disease. Other causes include inflammation (arthritis) and neurologic conditions. Sometimes the cause of leg length discrepancy is unknown, particularly in cases involving underdevelopment of the inner or outer side of the leg, or partial overgrowth of one side of the body. These conditions are usually present at birth, but the leg length difference may be too small to be detected. As the child grows, the leg length discrepancy increases and becomes more noticeable. In underdevelopment, one of the two bones between the knee and the ankle is abnormally short. There also may be related foot or knee problems. Hemihypertrophy (one side too big) or hemiatrophy (one side too small) are rare leg length discrepancy conditions. In these conditions, the arm and leg on one side of the body are either longer or shorter than the arm and leg on the other side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This is known as an "idiopathic" difference.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
A personalized approach to leg length discrepancy treatment works best for each patient. Your child's doctor will consider many factors when deciding on a course of treatment for this condition. Such factors can include your child's age, extent of the leg length discrepancy, medical history, how your child tolerates certain treatments and procedures, your child's health and prognosis, growth rate, and parental preferences. There is no cookie cutter treatment for each child, or even each centimeter of leg difference. Once all of these factors have been carefully considered, your child's physician will come up with an appropriate course of care. In situations of a very small leg length discrepancy, no treatment, only periodic medical evaluation, may be necessary.
how to grow taller at 17
Surgical Treatment
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.
Mortons Neuroma Prevention
Overview
 Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.
Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.
Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Episodes of pain are intermittent. Patients may experience 2 attacks in a week and then none for a year. Recurrences are variable and tend to become more frequent. Between attacks, no symptoms or physical signs occur. Two neuromas coexist on the same foot about 2-3% of the time. Other diagnoses should be considered when 2 or more areas of tenderness are present.
Diagnosis
The doctor will ask about your symptoms and medical history. A physical exam will be done. Initial diagnosis of Morton's neuroma is based on your description of the type and location of pain and discomfort in the foot. The diagnosis will be confirmed by a physical exam of the foot, including checking for mechanical abnormalities in the foot, squeezing the side of the foot, which will usually cause pain when Morton's neuroma is present. Examination of your shoes to check for excess wear in parts of the shoe, check to see whether the shoes are too tight. Imaging tests evaluate the foot and surrounding structures. This may be done with X-ray, MRI scan, Ultrasound. Injections of local anesthetic can also be used for diagnosis.
Non Surgical Treatment
Nonsurgical treatment is tried first. Your doctor may recommend any of the following. Padding and taping the toe area, shoe inserts, changes to footwear, for example wearing shoes with wider toe boxes or flat heels, Anti-inflammatory medicines taken by mouth or injected into the toe area, nerve blocking medicines injected into the toe area, other painkillers, physical therapy. Anti-inflammatories and painkillers are not recommended for long-term treatment. In some cases, surgery is needed to remove the thickened tissue and inflammed nerve. This helps relieve pain and improve foot function. Numbness after surgery is permanent.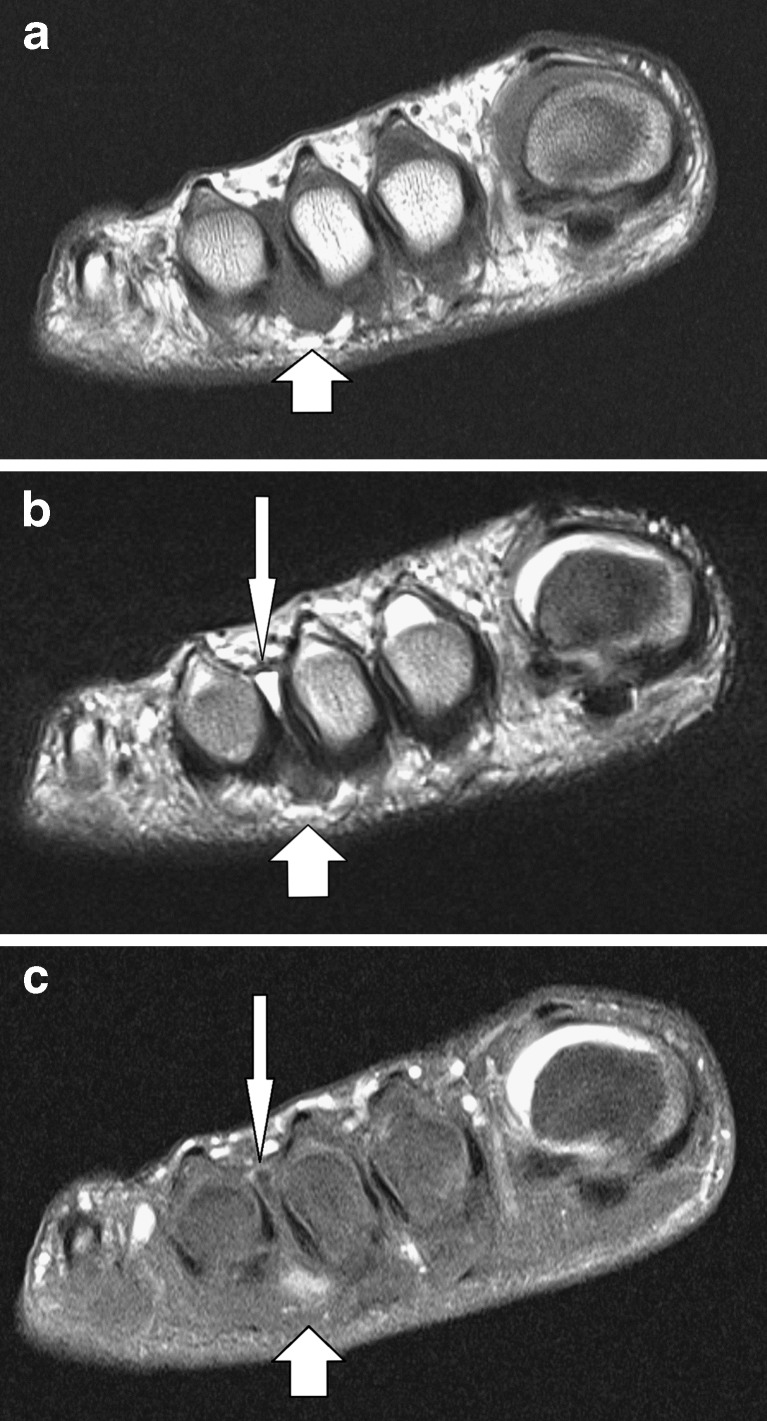
Surgical Treatment
If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet.
Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Episodes of pain are intermittent. Patients may experience 2 attacks in a week and then none for a year. Recurrences are variable and tend to become more frequent. Between attacks, no symptoms or physical signs occur. Two neuromas coexist on the same foot about 2-3% of the time. Other diagnoses should be considered when 2 or more areas of tenderness are present.
Diagnosis
The doctor will ask about your symptoms and medical history. A physical exam will be done. Initial diagnosis of Morton's neuroma is based on your description of the type and location of pain and discomfort in the foot. The diagnosis will be confirmed by a physical exam of the foot, including checking for mechanical abnormalities in the foot, squeezing the side of the foot, which will usually cause pain when Morton's neuroma is present. Examination of your shoes to check for excess wear in parts of the shoe, check to see whether the shoes are too tight. Imaging tests evaluate the foot and surrounding structures. This may be done with X-ray, MRI scan, Ultrasound. Injections of local anesthetic can also be used for diagnosis.
Non Surgical Treatment
Nonsurgical treatment is tried first. Your doctor may recommend any of the following. Padding and taping the toe area, shoe inserts, changes to footwear, for example wearing shoes with wider toe boxes or flat heels, Anti-inflammatory medicines taken by mouth or injected into the toe area, nerve blocking medicines injected into the toe area, other painkillers, physical therapy. Anti-inflammatories and painkillers are not recommended for long-term treatment. In some cases, surgery is needed to remove the thickened tissue and inflammed nerve. This helps relieve pain and improve foot function. Numbness after surgery is permanent.
Surgical Treatment
If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet.
What Are The Major Causes Of Inferior Calcaneal Spur

Overview
The two most common causes of pain in the bottom of the heel, the arch, or both the heel and the arch, are heel spurs and plantar fasciitis. A Heel Spur is a piece of calcium or bone that sticks out from the bottom of the heel bone, and lies within the fibers of the plantar fascia. When walking, the spur digs into the plantar fascia and causes small micro-tears in the plantar fascia. This produces inflammation and pain in the heel, which at times may radiate into the arch.
Causes
Heel spurs under the sole of the foot (plantar area) are associated with inflammation of the plantar fascia (fasciitis), the "bowstring-like" tissue stretching underneath the sole that attaches at the heel. Plantar heel spurs cause localized tenderness and pain made worse when stepping down on the heel. Heel spurs and plantar fasciitis can occur alone or be related to underlying diseases that cause arthritis (inflammation of the joints), such as reactive arthritis (formerly called Reiter's disease), ankylosing spondylitis, and diffuse idiopathic skeletal hyperostosis. It is important to note that heel spurs may cause no symptoms at all and may be incidentally discovered during X-ray exams taken for other purposes.

Symptoms
Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain.
Diagnosis
Your doctor will review your medical history and examine your foot. X-rays are used to identify the location and size of the heel spur.
Non Surgical Treatment
There are both conservative and surgical heel spur treatment options. Because the heel pain caused by heel spurs is symptomatic of inflammation, the first step is to ice the area in hopes to reduce the inflammation. The next step is to see our orthopedic specialist to prescribe an appropriate treatment plan. Some conservative treatment options might include Anti-inflammatory medications. Shoe orthotics. Shoe inserts. If conservative treatments are not working, surgery may be required to remove the heel spur. As in all cases of heel pain, it is important to see an orthopedic doctor who specializes in foot and ankle pain.
Surgical Treatment
In some cases, heel spurs are removed by surgery after an X-ray. While the surgery is typically effective, it?s a timely and expensive procedure. Even after surgery, heel spurs can re-form if the patient continues the lifestyle that led to the problem. These reasons are why most people who develop painful heel spurs begin looking for natural remedies for joint and bone pain. Surgery isn?t required to cure a heel spur. In fact, more than 90 percent of people get better with nonsurgical treatments. If nonsurgical methods fail to treat symptoms of heel spurs after 12 months, surgery may be necessary to alleviate pain and restore mobility.
Prevention
Walk around before you buy shoes. Before you purchase your shoes, do the following. Re-lace the shoes if you're trying on athletic shoes. Start at the farthest eyelets and apply even pressure to the laces as you come closer to the tongue of the shoe. Make sure that you can wiggle your toes freely inside of the shoe. Also, make sure that you have at enough space between your tallest toe and the end of the shoe. You should have room equal to about the width of your thumb in the tip of your shoe. Walk around to make sure that the shoe has a firm grip on your heel without sliding up and down. Walk or run a few steps to make sure your shoes are comfortable. Shoes that fit properly require no break-in period.
Heel Spur Symtoms
Overview
Approximately 10 per cent of the population may have heel spurs without any heel pain. Whilst recent research has raised the question of whether or not heel spurs are the result of the body trying to increase its base of support, heel spurs are still considered to be the result from strain on the muscles of the foot (in particular the plantar fascia). This may result from a biomechanical imbalance, such as over pronation.
Causes
A strong band of sinew (plantar fascia) stretches across the sole of the foot below the surface of the skin and is attached to a point in the middle of the under surface of the heel bone. With repeated activity on our feet, the plantar fascia can become tight and cause persistent traction (tugging) on its attachment point into the heel bone, and inflammation and pain may develop at this site. This painful condition is known as plantar fasciitis. Sometimes a ?spur? develops at the site of this traction on the bone and protrudes into the surrounding tissue. This is a heel spur.

Symptoms
Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain.
Diagnosis
Diagnosis is made using a few different technologies. X-rays are often used first to ensure there is no fracture or tumor in the region. Then ultrasound is used to check the fascia itself to make sure there is no tear and check the level of scar tissue and damage. Neurosensory testing, a non-painful nerve test, can be used to make sure there is not a local nerve problem if the pain is thought to be nerve related. It is important to remember that one can have a very large heel spur and no plantar fasciitis issues or pain at all, or one can have a great deal of pain and virtually no spur at all.
Non Surgical Treatment
The key is to identify what is causing excessive stretching of the plantar fascia. When the cause is over-pronation (flat feet), an orthotic with rearfoot posting and longitudinal arch support will help reduce the over-pronation and thus allow the condition to heal. Other common treatments for heel spurs include Stretching exercises. Losing weight. Wearing shoes that have a cushioned heel that absorbs shock. Elevating the heel with the use of a heel cradle, heel cup, or orthotics. For example, heel cradles and heel cups provide extra comfort and cushion to the heel, reducing the amount of shock and shear forces experienced from everyday activities.
Surgical Treatment
Sometimes bone spurs can be surgically removed or an operation to loosen the fascia, called a plantar fascia release can be performed. This surgery is about 80 percent effective in the small group of individuals who do not have relief with conservative treatment, but symptoms may return if preventative measures (wearing proper footwear, shoe inserts, stretching, etc) are not maintained.
Prevention
Heel spurs and plantar fasciitis can only be prevented by treating any underlying associated inflammatory disease.